Mitochondrial Dysfunction: The Hidden Energy Crisis in Chronic Illness
Uncover how mitochondrial dysfunction drives chronic illness. Learn what the research shows about its causes and how to restore function. Read more now!
Mitochondrial Dysfunction: The Hidden Energy Crisis in Chronic Illness
Mitochondrial dysfunction sits at the center of some of medicine's most complex and poorly understood chronic conditions, yet it rarely gets the attention it deserves. When these microscopic structures inside your cells stop producing energy efficiently, the consequences ripple across every organ system in the body, contributing to conditions as varied as Parkinson's disease, chronic fatigue, and autoimmune disorders. This article breaks down what the research actually shows about how mitochondria fail, why that failure drives chronic illness, and what current evidence says about restoring their function.
What is Mitochondrial Dysfunction and Why is it an Energy Crisis?
Mitochondrial dysfunction occurs when mitochondria, the organelles responsible for producing the vast majority of a cell's usable energy, fail to operate at the capacity the body requires. Every tissue and organ depends on a continuous supply of adenosine triphosphate (ATP), the molecule that powers virtually every biological process. When that supply falters, cells can't maintain their basic functions, and the downstream effects ripple through entire organ systems.
The Cellular Powerhouses Explained
Mitochondria are double-membraned structures found in nearly every human cell. Their inner membrane is folded into structures called cristae, which dramatically increase the surface area available for energy production. Through a process known as oxidative phosphorylation, electrons derived from nutrients pass along a series of protein complexes embedded in that membrane. This electron transport chain drives the synthesis of ATP, converting the chemical energy stored in food into a form cells can actually use. A single cardiac muscle cell can contain more than 5,000 mitochondria, reflecting just how energy-intensive sustained organ function really is.
Energy metabolism at the cellular level is therefore tightly linked to mitochondrial integrity. When the inner membrane is damaged, when key enzyme complexes are deficient, or when the mitochondrial genome carries mutations, ATP output drops. The cell must then make difficult trade-offs, prioritizing survival functions over repair, signaling, and specialized tasks.
The Energy Deficit: A Systemic Impact
The term "energy crisis" isn't an exaggeration. Tissues with the highest energy demands, including the brain, heart, skeletal muscle, and kidneys, are the first to show signs of dysfunction when ATP production declines. Neurons, for example, rely almost entirely on oxidative phosphorylation and have very limited capacity to switch fuel sources. A measurable drop in mitochondrial output can therefore translate quickly into cognitive fog, muscle weakness, or cardiac irregularities.
This is why the dysfunction is so often hidden in plain sight. Fatigue, exercise intolerance, and poor concentration are easy to attribute to lifestyle factors or stress. Yet in many chronic illnesses, these symptoms trace back to a genuine cellular energy shortage rather than a behavioral cause. Researchers at the National Institutes of Health have documented how impaired mitochondrial output contributes to a broad spectrum of conditions, underscoring why clinicians increasingly treat mitochondrial health as a foundational consideration rather than a niche concern.
Understanding this cellular energy deficit is the first step toward recognizing why so many chronic conditions share overlapping symptoms, and why addressing root-level mitochondrial health can shift outcomes in ways that symptom-focused approaches often cannot.
What are the Causes and Mechanisms of Mitochondrial Dysfunction?
Mitochondrial dysfunction arises from a complex interplay of inherited genetics, environmental exposures, and acquired cellular damage. No single cause tells the full story. Understanding the distinct pathways helps clarify why this condition presents so differently across patients and why identifying the root driver matters for effective care.
Genetic Predispositions and Acquired Factors
Genetics accounts for a significant share of cases. Mutations can originate in either nuclear DNA or mitochondrial DNA itself, and both inheritance patterns are well-documented in the research literature. Maternally inherited mutations, for instance, pass directly through the mitochondrial genome and can affect multiple family members across generations. The National Human Genome Research Institute notes that mitochondrial DNA is particularly vulnerable to mutation because it lacks the protective histones found around nuclear DNA and has less efficient repair mechanisms.

Beyond genetics, acquired factors play an equally important role. Chronic exposure to environmental toxins, including heavy metals, pesticides, and certain industrial chemicals, can directly impair the electron transport chain. Some prescription medications, notably statins and certain antiretrovirals, are also associated with mitochondrial damage as a side effect. Nutritional deficiencies in coenzyme Q10, B vitamins, magnesium, and lipoic acid deprive the mitochondria of the cofactors they need to generate ATP efficiently. Persistent viral or bacterial infections add another layer of stress, as pathogens can hijack mitochondrial signaling or trigger immune responses that collaterally damage mitochondrial membranes. For a deeper look at how hidden environmental exposures contribute to cellular damage, this functional medicine perspective on environmental toxicity offers useful clinical context.
The Role of Oxidative Stress and Free Radicals
Oxidation is a normal byproduct of energy production, but when free radical output exceeds the cell's antioxidant defenses, the resulting oxidative stress becomes destructive. Free radicals attack mitochondrial membranes, damage proteins within the respiratory chain, and mutate mitochondrial DNA. This creates a self-amplifying cycle: impaired mitochondria produce even more reactive oxygen species, which cause further structural damage and reduce energy output further. Research published through the NCBI confirms that this feedback loop is a central mechanism in many chronic degenerative conditions.
Chronic Inflammation and Mitochondrial Health
Persistent inflammation signals the immune system to release cytokines that directly suppress mitochondrial respiration. This stress inflammation response, while protective in the short term, becomes damaging when it persists for weeks or months. Pro-inflammatory cytokines such as TNF-alpha and interleukin-6 interfere with Complex I of the electron transport chain, reducing ATP synthesis and promoting dysregulation of cellular energy supply. The result is a state where inflammation and mitochondrial damage reinforce each other, deepening fatigue and accelerating tissue breakdown across multiple organ systems.
How Does Mitochondrial Dysfunction Impact Chronic Illnesses?
When mitochondrial dysfunction persists across tissues and organ systems, the downstream effects reach far beyond simple fatigue. Cells that cannot generate sufficient ATP begin to malfunction, triggering a cascade that underlies some of the most complex and treatment-resistant diseases clinicians encounter today. The conditions discussed below share a common thread: compromised mitochondrial energy output that amplifies cellular stress and drives disease progression.
Neurological and Neurodegenerative Disorders
Neurons are among the most energy-demanding cells in the body, making them acutely vulnerable when mitochondrial output drops. Research published in Nature Reviews Neuroscience has consistently linked impaired mitochondrial function to the accumulation of toxic protein aggregates seen in Alzheimer's and Parkinson's diseases. In Alzheimer's, reduced mitochondrial activity in hippocampal neurons precedes significant amyloid plaque formation, suggesting the energy deficit is an early driver rather than a late consequence. In Parkinson's, Complex I deficiency within the substantia nigra leads to dopaminergic neuronal loss. Both examples illustrate how neurodegenerative diseases can be understood, in part, as failures of mitochondrial energy supply to neurons that simply cannot survive on reduced output.
The link between mitochondrial dysfunction and neurodegenerative diseases also involves impaired calcium signaling, defective mitophagy (the clearance of damaged mitochondria), and elevated reactive oxygen species, all of which accelerate neuronal death and synaptic decline.
Autoimmune Conditions and Systemic Disease
Impaired mitochondria don't just starve cells of energy; they also release damage-associated molecular patterns (DAMPs) that activate innate immune receptors. This immune dysregulation is a key mechanism linking mitochondrial health to autoimmune diseases such as lupus, multiple sclerosis, and rheumatoid arthritis. When mitochondrial DNA leaks into the cytoplasm or extracellular space, it mimics bacterial DNA and triggers inflammatory signaling pathways, including the cGAS-STING axis. Studies in patients with systemic lupus erythematosus have documented elevated circulating mitochondrial DNA, pointing to a measurable biomarker of this process. For anyone interested in how environmental exposures compound this immune burden, the functional medicine perspective outlined in this article on environmental toxicity provides useful clinical context.
Lupus: Neutrophil extracellular traps enriched with mitochondrial DNA amplify autoantibody production.
Multiple sclerosis: Axonal degeneration correlates with mitochondrial respiratory chain defects in demyelinated lesions.
Rheumatoid arthritis: Synovial fibroblasts show elevated mitochondrial reactive oxygen species that sustain inflammatory joint destruction.
The Intersection with Aging
Mitochondrial decline is widely regarded as a hallmark of biological aging. The inflammation aging process, sometimes called "inflammaging," describes the chronic low-grade inflammatory state that accumulates as mitochondrial quality control deteriorates over decades. Damaged mitochondria that escape mitophagy continue to generate reactive oxygen species, sustaining a background of cellular stress that accelerates tissue aging across the heart, brain, and musculoskeletal system. In people with primary mitochondrial disorders, this trajectory is compressed: tissues age at a rate disproportionate to chronological years, and age-related diseases appear earlier. Caloric restriction studies in model organisms consistently show that preserving mitochondrial efficiency slows measurable markers of aging, reinforcing the direct relationship between mitochondrial health and longevity.
How Do You Recognize and Diagnose Mitochondrial Dysfunction?
Diagnosing Mitochondrial Dysfunction is notoriously difficult. Unlike conditions with a single, definitive test, this form of dysfunction presents differently across patients, often mimicking other diseases and delaying accurate identification by years. A comprehensive, multi-disciplinary approach is essential, combining clinical judgment with specialized laboratory and genetic analysis to reach a confident diagnosis of mitochondrial disease.
Diverse Clinical Manifestations
One reason diagnosis is so challenging is that mitochondria power virtually every organ system, so symptoms can appear almost anywhere. A patient may present with unexplained fatigue, muscle weakness, recurrent headaches, cognitive fog, hearing loss, or gastrointestinal dysmotility, sometimes all at once. Early symptoms are particularly non-specific: low energy and exercise intolerance are easily attributed to poor sleep or stress. Clinicians are trained to look for a pattern called "multi-system involvement," where seemingly unrelated complaints across neurological, cardiac, and metabolic domains point toward a shared underlying cause. When two or more organ systems are affected without a clear explanation, mitochondrial involvement moves higher on the differential diagnosis list.
Environmental exposures can also confuse the picture. As discussed in the context of environmental toxicity and functional medicine, hidden toxin burdens can produce overlapping symptoms, making it harder to isolate a mitochondrial root cause without a thorough patient history.
Diagnostic Tools and Biomarkers
When clinical findings raise suspicion, physicians draw on several specialized tests. Blood and urine metabolic panels measure lactate, pyruvate, and organic acids, which can reveal impaired cellular respiration. Elevated lactate-to-pyruvate ratios, for instance, are a recognized marker of respiratory chain dysfunction. A muscle biopsy with electron microscopy and enzyme activity assays for the respiratory chain complexes remains one of the most informative investigations, though it is invasive and requires an experienced laboratory to interpret accurately.
Genetics plays a central role in confirming a diagnosis. Next-generation sequencing panels now test hundreds of nuclear and mitochondrial genes simultaneously, identifying both inherited and de novo variants. Because genetics also informs prognosis and family counseling, many specialists recommend whole-exome sequencing when panel tests are inconclusive. Advanced neuroimaging, particularly MRI spectroscopy, can detect abnormal metabolite accumulation in brain tissue, adding another layer of evidence. Taken together, these tools build a diagnostic picture that no single test could provide alone.
What are the Common Symptoms of Mitochondrial Disease?
Symptoms of Mitochondrial Dysfunction span virtually every organ system, because cells throughout the body depend on a steady ATP supply. When that supply falters, tissues with the highest energy demands, including the brain, muscles, heart, and eyes, tend to show signs first. The specific pattern of symptoms often reflects which mitochondrial complex in the electron transport chain is impaired, making the clinical picture highly variable from one person to the next.

Systemic Symptoms and Their Impact
The most reported complaints in mitochondrial disease are persistent fatigue, muscle weakness, and poor exercise tolerance. These arise directly from inadequate ATP production in skeletal muscle. Patients often describe hitting an energy "wall" far sooner than peers, with recovery taking days rather than hours. Beyond muscles, the heart can develop cardiomyopathy or arrhythmias when cardiac cells cannot sustain their contractile workload. Gastrointestinal involvement is also common: dysmotility, nausea, and poor nutrient absorption reflect the high metabolic demands of gut smooth muscle and the enteric nervous system.
Neurological symptoms deserve particular attention. Cognitive fog, developmental delays, seizures, and stroke-like episodes all point to neuronal energy failure. Hearing loss appears frequently as well, because cochlear hair cells rank among the most metabolically active in the body. Endocrine disruption, including diabetes and growth failure, rounds out the systemic picture, since hormonal signaling relies on energy-intensive cellular machinery.
The Spectrum of Neuropathies
Nerve tissue is especially vulnerable when mitochondria underperform, and the resulting neuropathies range from mild sensory disturbance to severe motor impairment. Peripheral neuropathies produce numbness, tingling, and weakness in the limbs, reflecting demyelination and axonal loss driven by energy deficits in Schwann cells and neurons alike. Central neuropathies can cause ataxia and spasticity when neuronal pathways in the brain and spinal cord are compromised.
Among the most clinically recognized presentations are optic neuropathies, particularly Leber hereditary optic neuropathy, which causes sudden, painless vision loss in young adults due to retinal ganglion cell death. Optic neuropathies linked to mitochondrial dysfunction highlight how selectively vulnerable high-demand tissues are. A thorough symptom review that includes visual changes, alongside the more familiar fatigue and weakness, is therefore essential when mitochondrial involvement is suspected.
Neuromuscular: fatigue, weakness, exercise intolerance, ataxia
Neurological: seizures, cognitive decline, stroke-like episodes, hearing loss
Cardiac: cardiomyopathy, arrhythmia
Gastrointestinal: dysmotility, nausea, malabsorption
Visual: optic neuropathies, ptosis, ophthalmoplegia
Endocrine: diabetes, growth failure, thyroid dysregulation
Can Mitochondrial Dysfunction Be Treated Effectively?
Treatment for Mitochondrial Dysfunction is genuinely possible, though it rarely follows a single, uniform path. Because the condition varies widely between individuals, in severity, affected tissues, and underlying cause, clinicians typically build a personalized protocol that combines pharmacological support, targeted supplementation, and meaningful lifestyle change. No single intervention corrects every aspect of impaired mitochondrial function, which is why a layered strategy tends to produce the best outcomes.

Current Treatment Approaches
Pharmacological interventions focus on targeting the specific biochemical bottlenecks that reduce ATP output. Physicians may prescribe cofactors such as riboflavin (B2) or thiamine (B1) when testing reveals deficiencies in the electron transport chain. Coenzyme Q10 (CoQ10) is among the most studied supplements for mitochondrial support; a review published in Molecular Syndromology found CoQ10 supplementation beneficial in several primary mitochondrial diseases, particularly those involving Complex I and III deficits. L-carnitine supports fatty acid transport into the mitochondrial matrix, while alpha-lipoic acid acts as both a cofactor and an antioxidant, reducing the oxidative load on already stressed cells. These supplements are not interchangeable; the right combination depends on a patient's specific biochemical profile and test results.
Beyond supplements, some patients benefit from medications that reduce secondary complications. Anti-seizure drugs, cardiac medications, and agents that lower lactate levels are used symptomatically, addressing the downstream effects of poor energy production rather than the root dysfunction itself. Identifying these therapeutic targets requires close collaboration between a specialist and the patient over time.
Lifestyle Interventions
Dietary strategy is a meaningful lever. A dietary approach rich in antioxidants and micronutrients, particularly magnesium, B vitamins, and polyphenols from vegetables and berries, directly supports mitochondrial enzyme function. Some clinicians also explore ketogenic or modified Atkins protocols for patients whose cells handle fat-derived fuels more efficiently than glucose, though this requires careful monitoring.
Exercise, perhaps counterintuitively, is one of the most evidence-backed interventions available. Aerobic and resistance training stimulate mitochondrial biogenesis through the PGC-1α pathway, encouraging cells to build new, healthier mitochondria. The key is graded progression: starting low and building slowly prevents the post-exertional crashes that many patients fear. Stress reduction through consistent sleep, mindfulness practices, and reducing toxic exposures also lowers the physiological burden on cells already struggling to meet energy demands. For a broader look at how environmental exposures compound this burden, the perspective in this functional medicine overview of environmental toxicity offers useful context.
CoQ10, L-carnitine, and B-vitamin cofactors are first-line supplemental supports
Graded aerobic exercise promotes new mitochondrial growth
Dietary quality and sleep directly affect cellular repair capacity
Symptom management (cardiac, neurological) runs alongside root-cause work
Effective treatment, then, is less about a single breakthrough and more about consistently reducing the stressors that worsen dysfunction while actively supplying the nutrients and stimuli that support repair.
What Role Do Oxidative Stress and Inflammation Play in Mitochondrial Health?
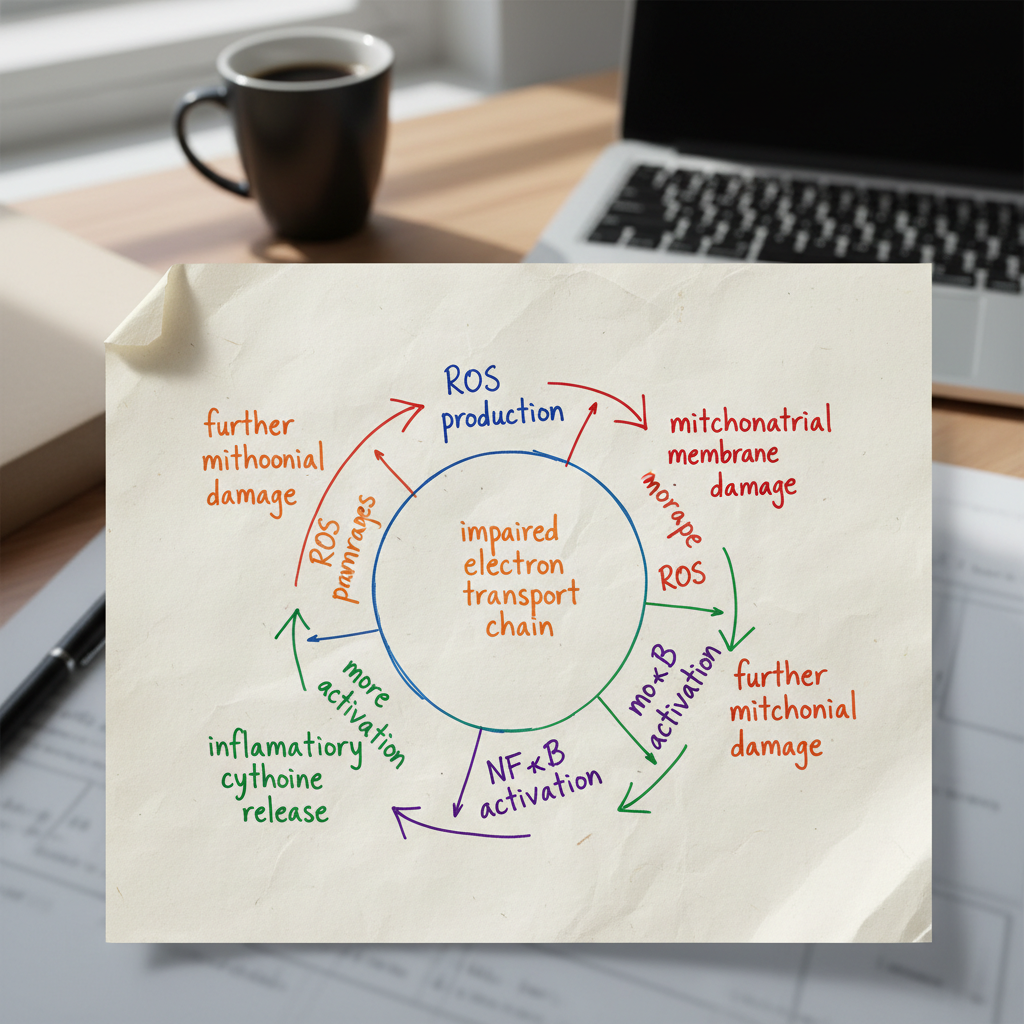
Oxidative stress and inflammation are not simply byproducts of cellular damage, they are active drivers of mitochondrial decline. When mitochondria generate ATP, a small fraction of electrons escape the electron transport chain and react with oxygen to form reactive oxygen species (ROS). Under normal conditions, antioxidant enzymes neutralize these molecules. When that balance tips, uncontrolled oxidation begins attacking mitochondrial membranes, proteins, and DNA, setting off a cascade that compounds over time.
The Vicious Cycle of Damage
The relationship between oxidative stress inflammation and mitochondrial damage is self-reinforcing. Excess ROS directly impair the electron transport chain complexes, reducing ATP output and causing mitochondria to leak even more free radicals. This ongoing oxidation then activates the NF-κB signaling pathway, one of the central switches for inflammatory gene expression. The result is a surge of pro-inflammatory cytokines, including TNF-α and IL-6, that further stress mitochondrial membranes and suppress mitochondrial biogenesis.
Damaged mitochondria also release mitochondrial DNA fragments into the cytoplasm. Because mitochondrial DNA shares structural features with bacterial DNA, the immune system reads these fragments as a threat and mounts an inflammatory response. This mechanism is particularly relevant in autoimmune conditions, where persistent stress inflammation keeps the immune system in a state of low-grade activation. Research published in Nature Reviews Immunology has documented this mitochondrial-to-immune signaling pathway as a key amplifier of systemic inflammation in chronic disease.
The cycle is especially damaging because inflammation itself suppresses the very enzymes, superoxide dismutase and glutathione peroxidase, that cells rely on to control oxidation. As those defenses weaken, oxidative stress inflammation intensifies, and Mitochondrial Dysfunction deepens. In chronic illnesses such as fibromyalgia, metabolic syndrome, and inflammatory bowel disease, this feedback loop is a consistent finding rather than an incidental one.
Anti-inflammatory and Antioxidant Strategies
Breaking this cycle requires targeting both arms simultaneously. On the nutritional side, compounds with well-documented antioxidant activity include CoQ10, alpha-lipoic acid, N-acetylcysteine (a glutathione precursor), and polyphenols such as resveratrol and curcumin. Curcumin, in particular, has been shown in peer-reviewed studies to inhibit NF-κB activation, directly reducing the inflammatory signaling that damages mitochondrial membranes.
Lifestyle factors carry equal weight. High-intensity interval training increases the expression of Nrf2, a transcription factor that upregulates the body's own antioxidant defenses. Reducing ultra-processed food intake lowers the substrate load for inflammatory prostaglandin production. Sleep, often underestimated, is the window during which mitochondrial quality control (mitophagy) removes the most compromised organelles. Addressing environmental toxin exposure is another lever; the functional medicine perspective outlined in this overview of environmental toxicity explains how biotoxin burden amplifies both oxidation and inflammatory load at the cellular level.
Combining targeted nutritional support with consistent lifestyle modifications gives the body the best chance of restoring the redox balance that healthy mitochondria depend on.
How Do Lifestyle and Dietary Choices Affect Mitochondrial Function?
What you eat, how you move, and how well you sleep all send direct signals to your cells' energy-producing machinery. These inputs can either support robust mitochondrial output or quietly accelerate the kind of dysfunction that compounds over time, particularly as aging progresses and cellular repair systems become less efficient.

Optimal Nutrition for Mitochondrial Health
Dietary pattern matters more than any single supplement. Ketogenic and low-glycemic diets reduce reliance on glucose oxidation, pushing cells toward fat-derived ketones, which generate fewer damaging free radicals per unit of ATP produced. Intermittent fasting adds another layer of benefit: periods of caloric restriction activate AMPK and SIRT1 pathways, both of which stimulate mitochondrial biogenesis, the process by which cells build new, functional mitochondria.
Specific micronutrients are non-negotiable. Coenzyme Q10 sits at the heart of the electron transport chain, and low levels correlate directly with impaired energy output. B vitamins (especially B2, B3, and B12) serve as essential cofactors for multiple enzymatic steps in ATP synthesis. Magnesium activates more than 300 enzymes, including those driving oxidative phosphorylation. Polyphenols found in berries, green tea, and dark leafy vegetables support antioxidant defenses that protect mitochondrial membranes from oxidative damage. A 2018 review in Nutrients confirmed that dietary polyphenols can upregulate mitochondrial biogenesis markers in human cell models.
Macronutrient balance also shapes energy efficiency. Excessive refined carbohydrates flood the system with glucose, overwhelming the electron transport chain and increasing free radical production. Prioritizing quality fats, adequate protein, and fiber-rich carbohydrates keeps metabolic flux steady and reduces the oxidative burden on mitochondria.
Exercise and Sleep: Beyond the Basics
Exercise is one of the most potent stimuli for mitochondrial adaptation. Endurance training, such as brisk walking, cycling, or swimming, increases mitochondrial density in muscle tissue by activating PGC-1α, the master regulator of biogenesis. High-intensity interval training (HIIT) produces similar or greater gains in less time, making it particularly practical. Resistance training complements both by preserving muscle mass, which declines with aging and takes mitochondrial capacity with it.
Sleep is where cellular repair actually happens. During deep sleep stages, cells clear damaged proteins and organelles through a process called mitophagy, selectively removing dysfunctional mitochondria before they can spread harm. Chronic poor sleep disrupts this process, allowing damaged components to accumulate. Adults who consistently sleep fewer than seven hours show measurably higher markers of oxidative stress the following day, according to research published in the Sleep Foundation's reviewed literature. Prioritizing sleep hygiene is, in practical terms, a direct investment in cellular energy capacity.
Key dietary supports: CoQ10, B vitamins, magnesium, polyphenols, and healthy fats
Exercise types: endurance training, HIIT, and resistance work each contribute distinct mitochondrial benefits
Sleep goal: seven to nine hours to support mitophagy and reduce oxidative load
What are the Emerging Therapeutic Targets and Future Directions for Mitochondrial Dysfunction?
Research into Mitochondrial Dysfunction is accelerating rapidly, with scientists identifying increasingly precise therapeutic targets that go well beyond general antioxidant support. The field now recognizes that correcting the underlying pathogenic mechanisms, rather than simply managing symptoms, is the most promising path forward for patients with both rare mitochondrial disease and common neurodegenerative conditions.

Innovative Pharmacological and Genetic Approaches
Several drug candidates are now targeting mitochondrial-specific pathways with measurable precision. MitoQ and Elamipretide (SS-31), for example, are designed to concentrate antioxidant activity directly inside the mitochondrial membrane, reducing oxidative damage at its source. Early clinical trials for Elamipretide in Barth syndrome and heart failure have shown improvements in exercise capacity, suggesting real translational potential. Meanwhile, published research in mitochondrial dysfunction neurodegenerative disease models supports the idea that targeting electron transport chain complexes can slow neuronal loss in conditions like Parkinson's disease.
Gene editing is another frontier gaining serious momentum. CRISPR-based tools are being refined to correct pathogenic point mutations in mitochondrial DNA, which standard nuclear gene-editing techniques cannot easily reach. Heteroplasmy shifting, a strategy that selectively reduces mutant mtDNA copies while preserving healthy ones, has shown early success in cell and animal models. Mitochondrial transplantation, where healthy mitochondria are transferred into damaged cells, has moved from laboratory curiosity to early human feasibility studies, particularly in cardiac surgery contexts.
Personalized Medicine and Precision Therapeutics
The broader trend in managing dysfunction is moving firmly toward individualized care. Because mitochondrial defects vary widely across patients, including differences in affected complexes, tissue distribution, and genetic background, a one-size approach consistently underperforms. Clinicians are beginning to use whole-genome sequencing alongside metabolomic profiling to map each patient's specific energy bottlenecks. This data-driven strategy allows treatment teams to select interventions matched to the precise deficit rather than applying a broad protocol.
Environmental contributors to mitochondrial decline, including toxin exposure, are also receiving renewed attention. Resources like this functional medicine perspective on environmental toxicity highlight how biotoxin burden can compound genetic vulnerabilities, reinforcing the case for personalized assessment. The outlook for patients is genuinely improving as these converging strategies move from bench to bedside.
How Does Mitochondrial Dysfunction Manifest as Neuropathies?
Nerve cells are among the most energy-hungry cells in the body. Neurons rely almost entirely on mitochondrial ATP production to maintain membrane potential, transmit signals, and repair cellular damage. When Mitochondrial Dysfunction disrupts that supply, neuronal integrity degrades, and neuropathies develop as a direct consequence. The link between dysfunction neurodegenerative processes and nerve damage is well-established in the research literature, making this one of the most clinically significant ways mitochondrial disease presents.
Impact on Peripheral and Central Nerves
In peripheral neuropathies, energy deficits impair axonal transport, the mechanism neurons use to shuttle proteins and organelles along their length. Without adequate ATP, this transport stalls, causing axons to degenerate from the tips inward. Patients typically experience numbness, burning pain, or weakness starting in the feet and hands. Central nervous system involvement follows a different pattern: neuronal loss in the brain and spinal cord can produce ataxia, cognitive decline, or spasticity. The distinction matters clinically because peripheral and central neuropathies often require different management strategies, even when both stem from the same underlying mitochondrial dysfunction neurodegenerative process.
Research published in the NCBI bookshelf on mitochondrial disorders confirms that dysfunction neurodegenerative pathology is frequently driven by impaired oxidative phosphorylation in high-demand neuronal populations, explaining why certain neuron types are disproportionately vulnerable.
Specific Examples of Mitochondrial Neuropathies
Several well-characterised neuropathies trace directly to mitochondrial pathology. MERRF (myoclonic epilepsy with ragged-red fibers) and MELAS (mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes) both involve severe neuronal energy failure. Among optic neuropathies, Leber hereditary optic neuropathy (LHON) is the most studied example of mitochondrial optic neuropathies, caused by point mutations in mitochondrial DNA that selectively destroy retinal ganglion cells. Dominant optic atrophy is another of the mitochondrial optic neuropathies, driven by mutations in the OPA1 gene that governs mitochondrial fusion. Both optic neuropathies can cause irreversible central vision loss, often in young adults, underscoring how rapidly these neuropathies can progress once neuronal energy supply collapses.
LHON: acute or subacute central vision loss, predominantly in males aged 15–35
MELAS: stroke-like episodes, seizures, and progressive neuronal decline
Peripheral sensorimotor neuropathy: length-dependent axonal degeneration with pain and weakness
Charcot-Marie-Tooth type 2A: linked to MFN2 mutations affecting mitochondrial dynamics
Early identification of these neuropathies allows clinicians to slow progression through targeted support, which connects directly to the treatment strategies discussed in earlier sections of this guide.
What is the Psychology of Living with Chronic Mitochondrial Conditions?
Living with a mitochondrial condition means contending with more than physical symptoms. The psychological weight of managing unpredictable fatigue, cognitive fog, and pain that others can't see creates a distinct emotional burden. For many patients, the gap between how they look and how they feel becomes a source of isolation, frustration, and self-doubt that compounds the physical reality of their condition.

Emotional and Mental Health Challenges
Research consistently shows that people living with chronic illness face elevated rates of depression and anxiety. In mitochondrial conditions specifically, this risk is compounded by a biological factor: systemic inflammation directly affects neurotransmitter pathways, lowering serotonin availability and disrupting mood regulation. A 2021 review published in Frontiers in Psychiatry found that inflammatory cytokines are strongly associated with depressive symptoms in patients with energy-limiting diseases. This means the psychological distress many patients experience isn't purely reactive. It has a physiological basis that deserves clinical attention alongside physical treatment.
Unpredictable symptom flares add another layer of difficulty. Planning becomes unreliable, relationships strain under the weight of cancelled commitments, and patients often internalize a sense of failure when they can't meet expectations. Grief over lost function, career limitations, and changed identity is common and legitimate.
Building Resilience and Support
Effective coping tends to involve a combination of professional support and peer connection. Cognitive behavioral therapy adapted for chronic illness helps patients reframe unhelpful thought patterns without minimizing their real experience. Acceptance and commitment therapy (ACT) has shown particular promise for improving quality of life when symptoms can't be fully controlled.
Patient communities, both in-person and online through organizations like the United Mitochondrial Disease Foundation, offer something clinical settings often can't: the validation of shared experience. Connecting with others navigating the same diseases reduces isolation and builds practical knowledge about day-to-day management strategies that genuinely help.
Frequently Asked Questions About Mitochondrial Dysfunction
These questions address the most common points of confusion about mitochondrial health, energy production, and the conditions that arise when cellular power generation breaks down. Each answer draws on concepts explored throughout this guide without repeating the full explanations already given.

What happens when mitochondria are not working properly?
Cells produce far less ATP than they need, so high-demand tissues, particularly the brain, heart, and muscles, begin to fail first. The downstream effects include persistent fatigue, cognitive fog, muscle weakness, and impaired organ function. Because virtually every cell relies on adequate ATP, the consequences of impaired mitochondria spread across multiple body systems simultaneously.
Why is mitochondrial dysfunction also called an energy crisis?
The term reflects the scale of the shortfall. When mitochondria underperform, the body cannot meet its baseline energy requirements, much like a city losing most of its power grid. Organs compensate briefly, but sustained deficits force cells into less efficient backup pathways, generating waste products that compound the damage over time.
What diseases are associated with mitochondrial dysfunction?
A broad range of diseases has clear mitochondrial links. Neurological conditions such as Alzheimer's, Parkinson's, and ALS are well documented, as are cardiovascular diseases, type 2 diabetes, and certain autoimmune conditions. Rare forms of mitochondrial disease, including MELAS syndrome and Leigh syndrome, represent the severe end of the spectrum, while milder impairment contributes to chronic fatigue and fibromyalgia.
Is mitochondrial dysfunction hereditary or acquired?
Both pathways exist. Inherited mutations in either mitochondrial or nuclear DNA can cause primary mitochondrial disease from birth or early childhood. Mitochondrial DNA depletion disorders, for example, arise from mutations that reduce the copy number of mitochondrial DNA, leading to a severe depletion syndrome that affects energy output in affected tissues. Acquired dysfunction, by contrast, develops through chronic exposure to toxins, persistent infections, poor nutrition, or prolonged oxidative stress, and can affect anyone at any age.
How do mitochondria produce energy for the body?
Mitochondria convert nutrients into ATP through a two-stage process. First, glucose and fatty acids are broken down to produce electron carriers. Those electrons then pass through the electron transport chain, a series of protein complexes embedded in the inner mitochondrial membrane, driving the synthesis of ATP through a process called oxidative phosphorylation. This chain reaction requires oxygen and key cofactors including CoQ10, B vitamins, and magnesium.
Are there specific dietary interventions for mitochondrial dysfunction?
Yes. Diets that reduce glucose spikes, such as low-carbohydrate or ketogenic approaches, shift fuel use toward fatty acids and ketones, which some research suggests are more efficient mitochondrial fuels. Antioxidant-rich foods help counter oxidative damage, while targeted nutrients including riboflavin, alpha-lipoic acid, and L-carnitine support specific steps in the ATP production pathway. Caloric restriction and time-restricted eating have also shown promise in stimulating mitochondrial renewal.
Can lifestyle changes improve mitochondrial function in chronic illness?
Evidence consistently supports aerobic and resistance exercise as stimuli for mitochondrial biogenesis, the process by which cells generate new, healthier mitochondria. Quality sleep allows repair of oxidative damage accumulated during waking hours. Stress management reduces cortisol-driven inflammation, which otherwise suppresses mitochondrial efficiency. These changes work gradually, so consistency over months matters more than short-term intensity.
What are the diagnostic tests for mitochondrial dysfunction?
Clinicians typically combine several approaches: blood and urine organic acid panels to detect abnormal metabolites, lactate-to-pyruvate ratios, and genetic screening for known pathogenic variants in both mitochondrial and nuclear DNA. Muscle biopsy with electron microscopy and enzyme activity assays remains a reference standard for confirming primary mitochondrial disease. Functional tests such as cardiopulmonary exercise testing can quantify real-world energy capacity when laboratory markers are inconclusive.
Conclusion
Mitochondrial dysfunction sits at the center of a vast web of chronic illness, quietly undermining cellular energy production long before a diagnosis is reached. Throughout this guide, we've traced that hidden crisis from its molecular origins through to its clinical consequences, covering everything from genetic risk factors and oxidative damage to the psychological weight of living with an unpredictable condition.

The breadth of impact is striking. Neurodegenerative conditions, autoimmune diseases, neuropathies, and metabolic disorders all share mitochondrial compromise as a common thread. That shared biology matters because it shifts the clinical conversation away from symptom suppression and toward root-cause investigation. When clinicians and patients understand what is actually failing at the cellular level, treatment decisions become sharper and more meaningful.
Research into therapeutic targets is accelerating. Gene editing, mitochondria-specific antioxidants, and personalized metabolic protocols are moving from laboratory settings into early clinical trials. None of these represents an overnight solution, but the trajectory is genuinely encouraging. In parallel, the lifestyle interventions covered here, including targeted nutrition, structured exercise, and sleep optimization, remain among the most accessible and evidence-supported tools available right now.
If you suspect that cellular energy failure may be contributing to your own health challenges, a functional medicine evaluation can help identify patterns that standard workups often miss. The path forward requires patience, good data, and a clinician willing to look beyond surface-level symptoms toward the mitochondria themselves.